

Definition Of A Perceptual Region
| Sensorineural hearing loss | |
|---|---|
 | |
| Cross department of the cochlea. | |
| Specialty | Otorhinolaryngology |
Sensorineural hearing loss (SNHL) is a blazon of hearing loss in which the root cause lies in the inner ear or sensory organ (cochlea and associated structures) or the vestibulocochlear nerve (cranial nerve VIII). SNHL accounts for about 90% of reported hearing loss[ citation needed ]. SNHL is normally permanent and can be mild, moderate, severe, profound, or total. Various other descriptors can be used depending on the shape of the audiogram, such as high frequency, low frequency, U-shaped, notched, peaked, or flat.
Sensory hearing loss often occurs as a effect of damaged or deficient cochlear hair cells.[ disputed ] Hair cells may be abnormal at nativity or damaged during the lifetime of an individual. There are both external causes of harm, including infection, and ototoxic drugs, too equally intrinsic causes, including genetic mutations. A common crusade or exacerbating factor in SNHL is prolonged exposure to environmental noise, or racket-induced hearing loss. Exposure to a single very loud noise such as a gun shot or flop nail can cause racket-induced hearing loss. Using headphones at loftier volume over time, or being in loud environments regularly, such as a loud workplace, sporting events, concerts, and using noisy machines can besides be a risk for noise-induced hearing loss.
Neural, or "retrocochlear", hearing loss occurs considering of impairment to the cochlear nerve (CVIII). This damage may bear on the initiation of the nervus impulse in the cochlear nerve or the transmission of the nerve impulse forth the nerve into the brainstem.
Most cases of SNHL present with a gradual deterioration of hearing thresholds occurring over years to decades. In some, the loss may eventually bear on large portions of the frequency range. Information technology may be accompanied by other symptoms such as ringing in the ears (tinnitus) and dizziness or lightheadedness (vertigo). The almost mutual kind of sensorineural hearing loss is historic period-related (presbycusis), followed by noise-induced hearing loss (NIHL).
Frequent symptoms of SNHL are loss of acuity in distinguishing foreground voices confronting noisy backgrounds, difficulty understanding on the phone, some kinds of sounds seeming excessively loud or shrill, difficulty understanding some parts of voice communication (fricatives and sibilants), loss of directionality of sound (particularly with high frequency sounds), perception that people mumble when speaking, and difficulty understanding spoken language. Similar symptoms are likewise associated with other kinds of hearing loss; audiometry or other diagnostic tests are necessary to distinguish sensorineural hearing loss.
Identification of sensorineural hearing loss is usually made past performing a pure tone audiometry (an audiogram) in which bone conduction thresholds are measured. Tympanometry and speech audiometry may be helpful. Testing is performed past an audiologist.
There is no proven or recommended treatment or cure for SNHL; management of hearing loss is ordinarily by hearing strategies and hearing aids. In cases of profound or total deafness, a cochlear implant is a specialised hearing aid that may restore a functional level of hearing. SNHL is at least partially preventable past fugitive environmental dissonance, ototoxic chemicals and drugs, and head trauma, and treating or inoculating against certain triggering diseases and weather like meningitis.
Signs and symptoms [edit]
Since the inner ear is not directly accessible to instruments, identification is by patient study of the symptoms and audiometric testing. Of those who nowadays to their dr. with sensorineural hearing loss, 90% written report having macerated hearing, 57% report having a plugged feeling in ear, and 49% report having ringing in ear (tinnitus). Well-nigh half report vestibular (vertigo) bug.
For a detailed exposition of symptoms useful for screening, a self-assessment questionnaire was developed by the American Academy of Otolaryngology, called the Hearing Handicap Inventory for Adults (HHIA). It is a 25-question survey of subjective symptoms.[one]
Causes [edit]
Sensorineural hearing loss may be genetic or acquired (i.e. every bit a upshot of illness, noise, trauma, etc.). People may have a hearing loss from nascence (congenital) or the hearing loss may come on later. Many cases are related to erstwhile historic period (age-related).
Genetic [edit]
Hearing loss can exist inherited. More than 40 genes have been implicated in the cause of deafness.[2] There are 300 syndromes with related hearing loss, and each syndrome may have causative genes.
Recessive, dominant, X-linked, or mitochondrial genetic mutations can bear upon the construction or metabolism of the inner ear. Some may be single point mutations, whereas others are due to chromosomal abnormalities. Some genetic causes give rise to a late onset hearing loss. Mitochondrial mutations can cause SNHL i.e. thousand.1555A>G, which makes the individual sensitive to the ototoxic furnishings of aminoglycoside antibiotics.
- The most common crusade of recessive genetic congenital hearing impairment in developed countries is DFNB1, also known as Connexin 26 deafness or GJB2-related deafness.
- The most mutual syndromic forms of hearing harm include (dominant) Stickler syndrome and Waardenburg syndrome, and (recessive) Pendred syndrome and Usher syndrome.
- Mitochondrial mutations causing deafness are rare: MT-TL1 mutations cause MIDD (Maternally inherited deafness and diabetes) and other conditions which may include deafness as part of the picture show.
- TMPRSS3 gene was identified by its association with both built and childhood onset autosomal recessive deafness. This gene is expressed in fetal cochleae and many other tissues, and is thought to be involved in the development and maintenance of the inner ear or the contents of the perilymph and endolymph. It was besides identified as a tumor associated gene that is overexpressed in ovarian tumors.
- Charcot–Marie–Tooth disease[three] an inherited neurological disorder with delayed onset that tin affect the ears every bit well as other organs. The hearing loss in this condition is often ANSD (auditory neuropathy spectrum disorder) a neural crusade of hearing loss.
- Muckle–Wells syndrome, a rare inherited autoinflammatory disorder, can lead to hearing loss.
- Autoimmune disease: although probably rare, it is possible for autoimmune processes to target the cochlea specifically, without symptoms affecting other organs. Granulomatosis with polyangiitis, an autoimmune condition, may precipitate hearing loss.
Built [edit]
- Infections:
- Built rubella syndrome, CRS, results from transplacental transmission of the rubella virus during pregnancy. CRS has been controlled by universal vaccination (MMR or MMRV vaccine).
- Cytomegalovirus (CMV) infection is the most common crusade of progressive sensorineural hearing loss in children. It is a mutual viral infection contracted past contact with infected bodily fluids such as saliva or urine and hands transmitted in nurseries and thus from toddlers to expectant mothers. CMV infection during pregnancy can affect the developing foetus and lead to learning difficulties as well as hearing loss.
- Toxoplasmosis, a parasitic disease affecting 23% of the population in the U.Due south., can cause sensorineural deafness to the fetus in utero.
- Hypoplastic auditory nerves or abnormalities of the cochlea. Abnormal development of the inner ear can occur in some genetic syndromes such every bit LAMM syndrome (labyrinthine aplasia, microtia and microdontia), Pendred syndrome, branchio-oto-renal syndrome, Accuse syndrome
- GATA2 deficiency, a group of several disorders caused past common defect, viz., familial or sporadic inactivating mutations in i of the 2 parental GATA2 genes. These autosomal dominant mutations crusade a reduction, i.east. a haploinsufficiency, in the cellular levels of the gene's production, GATA2. The GATA2 protein is a transcription factor critical for the embryonic development, maintenance, and functionality of blood-forming, lympathic-forming, and other tissue-forming stem cells. In effect of these mutations, cellular levels of GATA2 are deficient and individuals develop over time hematological, immunological, lymphatic, and/or other disorders. GATA2 deficiency-induced abnormalities in the lymphatic organisation are proposed to be responsible for a failure in generating the perilymphatic space around the inner ear's semicircular canals, which in plough underlies the development of sensorineural hearing loss.[iv] [five]
Presbycusis [edit]
Progressive historic period-related loss of hearing acuity or sensitivity can start every bit early every bit age 18, primarily affecting the high frequencies, and men more than than women.[6] Such losses may not become credible until much later in life. Presbycusis is by far the dominant cause of sensorineural hearing loss in industrialized societies. A study conducted in Sudan, with a population costless from loud noise exposures, found significantly less cases of hearing loss when compared with age-matched cases from an industrialized land.[7] Similar findings were reported by a study conducted of a population from Easter island, which reported worse hearing among those that spent time in industrialized countries when compared with those that never left the island.[eight] Researchers have argued that factors other than differences in dissonance exposure, such equally genetic make upwards, might also have contributed to the findings.[9] Hearing loss that worsens with age but is caused by factors other than normal aging, such as racket-induced hearing loss, is not presbycusis, although differentiating the individual effects of multiple causes of hearing loss can be difficult. One in three persons have significant hearing loss by age 65; by age 75, ane in two. Age-related hearing loss is neither preventable nor reversible.
Noise [edit]
Most people living in mod society accept some degree of progressive sensorineural (i.e. permanent) noise-induced hearing loss (NIHL) resulting from overloading and damaging the sensory or neural appliance of hearing in the inner ear. NIHL is typically a drib-out or notch centered at 4000 Hz. Both intensity (SPL) and duration of exposure, and repetitive exposure to unsafe levels of noise contribute to cochlear damage that results in hearing loss. The louder the noise is, the shorter the safe amount of exposure is. NIHL can be either permanent or temporary, called a threshold shift. Unsafe levels of racket tin can be as niggling as 70 dB (well-nigh twice as loud as normal conversation) if there is prolonged (24-hour) or continuous exposure. 125 dB (a loud rock concert is ~120 dB) is the pain level; sounds above this level cause instant and permanent ear impairment.
Noise and ageing are the primary causes of presbycusis, or age-related hearing loss, the near common kind of hearing loss in industrial lodge.[10] [ commendation needed ] The dangers of environmental and occupational dissonance exposure are widely recognized. Numerous national and international organizations take established standards for safe levels of exposure to dissonance in industry, the environs, military, transportation, agriculture, mining and other areas.[Note 1] Sound intensity or sound pressure level (SPL) is measured in decibels (dB). For reference:
| db Level | Example |
|---|---|
| 45 dB | Ambient noise level around the domicile |
| 60 dB | Quiet function |
| threescore–65 dB | Normal conversation |
| seventy dB | City street noise at 25'[ clarification needed ] or average Tv set audio |
| 80 dB | Noisy role |
| 95–104 dB | Nightclub dance floor |
| 120 dB | Shut by thunder or a loud rock concert |
| 150–160 dB | Gunshot from a handheld gun |
An increase of 6 dB represents a doubling of the SPL, or energy of the sound moving ridge, and therefore its propensity to crusade ear harm. Because human ears hear logarithmically, not linearly, it takes an increase of ten dB to produce a sound that is perceived to be twice as loud. Ear harm due to dissonance is proportional to sound intensity, not perceived loudness, so it's misleading to rely on subjective perception of loudness as an indication of the risk to hearing, i.e. it tin can significantly underestimate the danger.
While the standards differ moderately in levels of intensity and duration of exposure considered prophylactic, some guidelines can be derived.[Note 2]
The condom amount of exposure is reduced by a factor of 2 for every exchange rate (iii dB for NIOSH standard or 5 dB for OSHA standard) increase in SPL. For example, the safe daily exposure amount at 85 dB (ninety dB for OSHA) is 8 hours, while the safe exposure at 94 dB(A) (nightclub level) is only 1 hour. Noise trauma can also cause a reversible hearing loss, called a temporary threshold shift. This typically occurs in individuals who are exposed to gunfire or firecrackers, and hear ringing in their ears after the consequence (tinnitus).
- Ambient environmental noise: Populations living near airports, railyards and train stations, freeways and industrial areas are exposed to levels of noise typically in the 65 to 75 dBA range. If lifestyles include significant outdoor or open up window conditions, these exposures over time can degrade hearing. U.S. Dept. of Housing and Urban Development sets standards for noise impact in residential and commercial construction zones. HUD'southward noise standards may exist constitute in 24 CFR Part 51, Subpart B. Environmental racket above 65 dB defines a racket-impacted area.
- Personal sound electronics: Personal audio equipment such as iPods (iPods often reach 115 decibels or higher), can produce powerful enough sound to cause pregnant NIHL.[11]
- Acoustic trauma: Exposure to a single event of extremely loud dissonance (such every bit explosions) tin also cause temporary or permanent hearing loss. A typical source of audio-visual trauma is a besides-loud music concert.
- Workplace noise: The OSHA standards 1910.95 Full general Industry Occupational Dissonance Exposure and 1926.52 Construction Manufacture Occupational Racket Exposure place the level of xc dB(A) for 8 hour exposure every bit the level necessary to protect workers from hearing loss.
Affliction or disorder [edit]
- Inflammatory
- Suppurative labyrinthitis or otitis interna (inflammation of the inner ear)
- Diabetes mellitus A recent written report found that hearing loss is twice as common in people with diabetes as it is in those who don't accept the disease. Also, of the 86 million adults in the U.Southward. who take prediabetes, the rate of hearing loss is 30 percent college than in those with normal blood glucose. It has not been established how diabetes is related to hearing loss. It is possible that the high blood glucose levels associated with diabetes cause harm to the pocket-size claret vessels in the inner ear, similar to the way in which diabetes can damage the optics and the kidneys. Similar studies take shown a possible link between that hearing loss and neuropathy (nerve damage).
- Tumor
- Cerebellopontine angle neoplasm (junction of the pons and cerebellum) – The cerebellopontine angle is the exit site of both the facial nervus(CN7) and the vestibulocochlear nervus(CN8). Patients with these tumors oftentimes have signs and symptoms respective to compression of both nerves.
- Acoustic neuroma (vestibular schwannoma) – benign tumour of Schwann cells affecting the vestibulocochlear nervus
- Meningioma – beneficial tumour of the pia and arachnoid mater
- Cerebellopontine angle neoplasm (junction of the pons and cerebellum) – The cerebellopontine angle is the exit site of both the facial nervus(CN7) and the vestibulocochlear nervus(CN8). Patients with these tumors oftentimes have signs and symptoms respective to compression of both nerves.
- Ménière'south disease – causes sensorineural hearing loss in the low frequency range (125 Hz to 1000 Hz). Ménière's affliction is characterized by sudden attacks of vertigo, lasting minutes to hours preceded by tinnitus, aural fullness, and fluctuating hearing loss. It is relatively rare and commonly over diagnosed.
- Bacterial meningitis e.one thousand. pneumococcal, meningococcal, haemophilus influenzae may damage the cochlea – Hearing loss is one of the most mutual after-furnishings of bacterial meningitis. It has been estimated that 30% of bacterial meningitis cases result in mild to profound hearing loss. Children are most at risk: seventy percentage of all bacterial meningitis occurs in immature children under the age of v.
- Viral
- AIDS and ARC patients frequently experience auditory organization anomalies.
- Mumps(epidemic parotitis) may result in profound sensorineural hearing loss (xc dB or more), unilaterally (ane ear) or bilaterally (both ears).
- Measles may result in auditory nervus impairment but more usually gives a mixed (sensorineural plus conductive) hearing loss, and can be bilaterally.
- Ramsay Chase syndrome type Ii (canker zoster oticus)
- Bacterial
- Syphilis is commonly transmitted from pregnant women to their fetuses, and about a third of the infected children volition eventually become deafened.
Ototoxic and neurotoxic drugs and chemicals [edit]
Some over-the-counter every bit well as prescription drugs and certain industrial chemicals are ototoxic. Exposure to these can issue in temporary or permanent hearing loss.
Some medications cause irreversible impairment to the ear, and are express in their utilize for this reason. The nearly of import group is the aminoglycosides (main fellow member gentamicin). A rare mitochondrial mutation, g.1555A>Thousand, tin can increment an individual'southward susceptibility to the ototoxic effect of aminoglycosides. Long term hydrocodone (Vicodin) corruption is known to crusade rapidly progressing sensorineural hearing loss, unremarkably without vestibular symptoms. Methotrexate, a chemotherapy amanuensis, is also known to cause hearing loss. In most cases hearing loss does not recover when the drug is stopped. Paradoxically, methotrexate is also used in the treatment of autoimmune-induced inflammatory hearing loss.
Various other medications may reversibly dethrone hearing. This includes loop diuretics, sildenafil (Viagra), high or sustained dosing of NSAIDs (aspirin, ibuprofen, naproxen, and various prescription drugs: celecoxib, etc.), quinine, and macrolide antibiotics (erythromycin, etc.). Cytotoxic agents such as carboplatinum, used to care for malignancies can give rise to a dose dependent SNHL, as can drugs such as desferrioxamine, used for haematological disorders such as thalassaemia; patients prescribed these drugs need to have hearing monitored.
Prolonged or repeated ecology or work-related exposure to ototoxic chemicals tin also effect in sensorineural hearing loss. Some of these chemicals are:
- butyl nitrite – chemic used recreationally known equally 'poppers'
- carbon disulfide – a solvent used equally a building block in many organic reactions
- styrene, an industrial chemic precursor of polystyrene, a plastic
- carbon monoxide, a poisonous gas resulting from incomplete combustion
- heavy metals: tin, pb, manganese, mercury
- hexane, an industrial solvent and one of the significant constituents of gasoline
- ethylbenzene, an industrial solvent used in the production of styrene
- toluene and xylene, highly poisonous petrochemical solvents. Toluene is a component of high-octane gasoline; xylene is used in the product of polyester fibers and resins.
- trichloroethylene, an industrial degreasing solvent
- Organophosphate pesticides
Head trauma [edit]
There can be damage either to the ear itself or to the primal auditory pathways that process the information conveyed past the ears. People who sustain caput injury are susceptible to hearing loss or tinnitus, either temporary or permanent. Contact sports similar football (U.S. NFL), hockey and cricket have a notable incidence of head injuries (concussions). In one survey of retired NFL players, all of whom reported one or more than concussions during their playing careers, 25% had hearing loss and 50% had tinnitus.[ citation needed ]
Perinatal conditions [edit]
These are much more than mutual in premature babies, especially those under 1500 g at birth. Premature birth tin be associated with bug that result in sensorineural hearing loss such as anoxia or hypoxia (poor oxygen levels), jaundice, intracranial haemorrhages, meningitis. Fetal alcohol syndrome is reported to cause hearing loss in upwards to 64% of infants born to alcoholic mothers, from the ototoxic result on the developing fetus, plus malnutrition during pregnancy from the excess alcohol intake.
Iodine deficiency / Hypothyroidism [edit]
Iodine deficiency and owned hypothyroidism are associated with hearing loss.[12] If a pregnant female parent has insufficient iodine intake during pregnancy it affects the development of the inner ear in the foetus leading to sensorineural deafness. This occurs in certain areas of the globe, such as the Himalayas, where iodine is deficient in the soil and thus the diet. In these areas at that place is a loftier incidence of owned goitre. This cause of deafness is prevented by adding iodine to salt.
Brain stroke [edit]
Brain stroke in a region affecting auditory role such every bit a posterior circulation infarct has been associated with deafness.
Pathophysiology [edit]
Sensory hearing loss is caused by abnormal structure or function of the pilus cells of the organ of Corti in the cochlea.[ disputed ] Neural hearing impairments are consequent upon impairment to the 8th cranial nerve (the vestibulocochlear nerve) or the auditory tracts of the brainstem. If higher levels of the auditory tract are affected this is known as cardinal deafness. Central deafness may present every bit sensorineural deafness simply should be distinguishable from the history and audiological testing.
Cochlear dead regions in sensory hearing loss [edit]
Hearing harm may be associated with damage to the hair cells in the cochlea. Sometimes at that place may exist complete loss of function of inner hair cells (IHCs) over a certain region of the cochlea; this is called a "dead region". The region can be defined in terms of the range of characteristic frequencies (CFs) of the IHCs and/or neurons immediately adjacent to the expressionless region.
Cochlear hair cells [edit]

Figure three: Cross-section of the cochlea.
Outer pilus cells (OHCs) contribute to the structure of the Organ of Corti, which is situated between the basilar membrane and the tectorial membrane within the cochlea (See Figure three). The tunnel of corti, which runs through the Organ of Corti, divides the OHCs and the inner hair cells (IHCs). OHCs are connected to the reticular laminar and the Deiters' cells. There are roughly twelve thousand OHCs in each human ear, and these are bundled in up to v rows. Each OHC has pocket-size tufts of 'hairs', or cilia, on their upper surface known as stereocilia, and these are besides arranged into rows which are graded in top. There are approximately 140 stereocilia on each OHC.[13]
The fundamental office of the OHCs and the IHCs is to function equally sensory receptors. The main function of the IHCs is to transmit sound information via afferent neurons. They do this past transducing mechanical movements or signals into neural activity. When stimulated, the stereocilia on the IHCs move, causing a flow of electrical current to laissez passer through the hair cells. This electric electric current creates activeness potentials within the connected afferent neurons.
OHCs are different in that they actually contribute to the active mechanism of the cochlea. They practise this by receiving mechanical signals or vibrations along the basilar membrane, and transducing them into electrochemical signals. The stereocilia constitute on OHCs are in contact with the tectorial membrane. Therefore, when the basilar membrane moves due to vibrations, the stereocilia bend. The direction in which they bend, dictates the firing charge per unit of the auditory neurons connected to the OHCs.[xiv]
The bending of the stereocilia towards the basal body of the OHC causes excitation of the pilus cell. Thus, an increment in firing charge per unit of the auditory neurons connected to the hair cell occurs. On the other mitt, the angle of the stereocilia away from the basal body of the OHC causes inhibition of the hair prison cell. Thus, a decrease in firing rate of the auditory neurons continued to the hair jail cell occurs. OHCs are unique in that they are able to contract and expand (electromotility). Therefore, in response to the electrical stimulations provided past the efferent nervus supply, they can change in length, shape and stiffness. These changes influence the response of the basilar membrane to audio.[13] [14] Information technology is therefore articulate that the OHCs play a major role in the agile processes of the cochlea.[13] The main function of the active machinery is to finely melody the basilar membrane, and provide information technology with a high sensitivity to tranquillity sounds. The active machinery is dependent on the cochlea being in good physiological condition. All the same, the cochlea is very susceptible to damage.[xiv]
Hair cell damage [edit]
SNHL is nearly usually caused by harm to the OHCs and the IHCs.[ disputed ] There are two methods by which they might become damaged. Firstly, the entire hair cell might dice. Secondly, the stereocilia might become distorted or destroyed. Damage to the cochlea can occur in several ways, for example by viral infection, exposure to ototoxic chemicals, and intense dissonance exposure. Harm to the OHCs results in either a less effective active mechanism, or information technology may non function at all. OHCs contribute to providing a high sensitivity to quiet sounds at a specific range of frequencies (approximately two–4 kHz). Thus, damage to the OHCs results in the reduction of sensitivity of the basilar membrane to weak sounds. Amplification to these sounds is therefore required, in club for the basilar membrane to respond efficiently. IHCs are less susceptible to damage in comparison to the OHCs. Nevertheless, if they go damaged, this will result in an overall loss of sensitivity.[14]
Neural tuning curves [edit]
Frequency selectivity [edit]
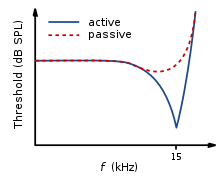
Figure 4: Neural tuning curve for normal hearing.
The traveling moving ridge along the basilar membrane peaks at dissimilar places forth it, depending on whether the sound is low or high frequency. Due to the mass and stiffness of the basilar membrane, low frequency waves peak in the apex, while high frequency sounds peak in the basal end of the cochlea.[13] Therefore, each position along the basilar membrane is finely tuned to a particular frequency. These specifically tuned frequencies are referred to as characteristic frequencies (CF).[14]
If a sound entering the ear is displaced from the feature frequency, and then the forcefulness of response from the basilar membrane will progressively lessen. The fine tuning of the basilar membrane is created past the input of two dissever mechanisms. The first mechanism existence a linear passive machinery, which is dependent on the mechanical construction of the basilar membrane and its surrounding structures. The second mechanism is a not-linear agile mechanism, which is primarily dependent on the functioning of the OHCs, and also the general physiological status of the cochlea itself. The base and noon of the basilar membrane differ in stiffness and width, which crusade the basilar membrane to reply to varying frequencies differently along its length. The base of operations of the basilar membrane is narrow and stiff, resulting in it responding best to loftier frequency sounds. The apex of the basilar membrane is wider and much less stiff in comparison to the base, causing information technology to respond best to depression frequencies.[fourteen]
This selectivity to certain frequencies can be illustrated by neural tuning curves. These demonstrate the frequencies a cobweb responds to, past showing threshold levels (dB SPL) of auditory nerve fibers every bit a function of unlike frequencies. This demonstrates that auditory nerve fibers respond all-time, and hence have better thresholds at the fiber's feature frequency and frequencies immediately surrounding it. The basilar membrane is said to be 'sharply tuned' due to the precipitous 'V' shaped curve, with its 'tip' centered at the auditory fibers characteristic frequency. This shape shows how few frequencies a fiber responds to. If it were a broader 'V' shape, it would be responding to more frequencies (Meet Figure four).[13]
IHC vs OHC hearing loss [edit]

Figure 5: Neural tuning curve for OHC loss. Adapted from.[14]

Figure 6: Neural tuning bend for OHC front row loss and IHC loss. Adjusted from.[xiv]
A normal neural tuning curve is characterised by a broadly tuned low frequency 'tail', with a finely tuned middle frequency 'tip'. Withal, where there is partial or consummate damage to the OHCs, but with unharmed IHCs, the resulting tuning curve would prove the emptying of sensitivity at the repose sounds. I.e. where the neural tuning curve would normally be most sensitive (at the 'tip') (See Effigy 5).[xiv]
Where both the OHCs and the IHCs are damaged, the resulting neural tuning curve would testify the elimination of sensitivity at the 'tip'. However, due to IHC damage, the whole tuning curve becomes raised, giving a loss of sensitivity across all frequencies (Encounter Figure vi). It is just necessary for the beginning row of OHCs to be damaged for the elimination of the finely tuned 'tip' to occur. This supports the idea that the incidence of OHC harm and thus a loss of sensitivity to quiet sounds, occurs more IHC loss.[14]
When the IHCs or role of the basilar membrane are damaged or destroyed, so that they no longer function as transducers, the result is a 'dead region'. Dead regions can be defined in terms of the characteristic frequencies of the IHC, related to the specific place along the basilar membrane where the expressionless region occurs. Assuming that in that location has been no shift in the characteristic frequencies relating to certain regions of the basilar membrane, due to the damage of OHCs. This often occurs with IHC damage. Dead regions can also be divers past the anatomical place of the non-operation IHC (such equally an "apical dead region"), or by the characteristic frequencies of the IHC next to the dead region.[15]
Expressionless region audiometry [edit]
Pure tone audiometry (PTA) [edit]
Expressionless regions touch on audiometric results, but mayhap not in the way expected. For example, it may exist expected that thresholds would not be obtained at the frequencies within the dead region, just would be obtained at frequencies adjacent to the dead region. Therefore, assuming normal hearing exists around the expressionless region, it would produce an audiogram that has a dramatically steep slope between the frequency where a threshold is obtained, and the frequency where a threshold cannot be obtained due to the dead region.[xv]

Figure 7: Response of the basilar membrane to a pure tone.

Figure 8: Response of the basilar membrane to a pure tone, when there is a expressionless region.
Nevertheless, it appears that this is non the case. Dead regions cannot be clearly constitute via PTA audiograms. This may be considering although the neurons innervating the dead region, cannot react to vibration at their feature frequency. If the basilar membrane vibration is large enough, neurons tuned to different characteristic frequencies such as those side by side to the dead region, will be stimulated due to the spread of excitation. Therefore, a response from the patient at the test frequency will exist obtained. This is referred to as "off-place listening", and is as well known as 'off-frequency listening'. This volition lead to a false threshold existence found. Thus, it appears a person has better hearing than they really do, resulting in a expressionless region beingness missed. Therefore, using PTA lone, it is impossible to identify the extent of a dead region (See Figure vii and 8).[15]
Consequently, how much is an audiometric threshold afflicted by a tone with its frequency inside a expressionless region? This depends on the location of the dead region. Thresholds at low frequency dead regions, are more inaccurate than those at college frequency dead regions. This has been attributed to the fact that excitation due to vibration of the basilar membrane spreads upwards from the upmost regions of the basilar membrane, more than than excitation spreads downwards from college frequency basal regions of the cochlea. This design of the spread of excitation is similar to the 'upward spread of masking' phenomenon. If the tone is sufficiently loud to produce enough excitation at the normally performance area of the cochlea, so that it is above that areas threshold. The tone will be detected, due to off-frequency listening which results in a misleading threshold.[15]
To help to overcome the event of PTA producing inaccurate thresholds inside dead regions, masking of the area beyond the dead region that is being stimulated can exist used. This means that the threshold of the responding surface area is sufficiently raised, so that it cannot detect the spread of excitation from the tone. This technique has led to the suggestion that a low frequency dead region may be related to a loss of 40-50 dB.[16] [17] Nevertheless, as one of the aims of PTA is to determine whether or not there is a dead region, it may exist difficult to appraise which frequencies to mask without the use of other tests.[15]
Based on research it has been suggested that a low frequency dead region may produce a relatively flat loss, or a very gradually sloping loss towards the college frequencies. As the expressionless region will be less detectable due to the upwards spread of excitation. Whereas, in that location may be a more obvious steeply sloping loss at high frequencies for a high frequency expressionless region. Although it is likely that the slope represents the less pronounced downward spread of excitation, rather than accurate thresholds for those frequencies with not-operation pilus cells. Mid-frequency dead regions, with a modest range, appear to have less effect on the patient's power to hear in everyday life, and may produce a notch in the PTA thresholds.[15] Although it is clear that PTA is not the best test to identify a dead region.[xviii]
Psychoacoustic tuning curves (PTC) and threshold equalizing dissonance (Ten) tests [edit]

Figure nine: Psychoacoustical tuning curve.
Although some debate continues regarding the reliability of such tests,[19] it has been suggested[ weasel words ]that psychoacoustic tuning curves (PTCs) and threshold-equalising noise (TEN) results may exist useful in detecting dead regions, rather than PTA. PTCs are similar to neural tuning curves. They illustrate the level of a masker (dB SPL) tone at threshold, as a part of deviation from eye frequency (Hz).[xiii] They are measured by presenting a stock-still depression intensity pure tone while too presenting a narrow-band masker, with a varying center frequency. The masker level is varied, and then that the level of masker needed to just mask the test signal is found for the masker at each middle frequency. The tip of the PTC is where the masker level needed to just mask the examination signal is the everyman. For normal hearing people this is when the masker center frequency is closest to the frequency of the test bespeak (See Figure 9).[18]
In the instance of dead regions, when the test signal lies within the boundaries of a dead region, the tip of the PTC will exist shifted to the edge of the dead region, to the expanse that is still functioning and detecting the spread of excitation from the signal. In the case of a low frequency expressionless region, the tip is shifted upwards indicating a depression frequency dead region starting at the tip of the curve. For a loftier frequency dead region, the tip is shifted down from the signal frequency to the functioning area below the dead region.[18] However, the traditional method of obtaining PTCs is not practical for clinical use, and it has been argued[ weasel words ] that TENs are not authentic plenty.[18] [19] A fast method for finding PTCs has been developed and it may provide the solution. However, more research to validate this method is required, earlier it can be accepted clinically.
Perceptual consequences of a dead region [edit]
Audiogram configurations are not good indicators of how a dead region will touch a person functionally, mainly due to individual differences.[14] For example, a sloping audiogram is oftentimes present with a expressionless region, due to the spread of excitation. However, the private may well exist affected differently from someone with a corresponding sloped audiogram acquired by partial damage to hair cells rather than a dead region. They will perceive sounds differently, yet the audiogram suggests that they have the same degree of loss. Huss and Moore investigated how hearing impaired patients perceive pure tones, and found that they perceive tones as noisy and distorted, more than (on average) than a person without a hearing impairment. However, they also found that the perception of tones equally being like noise, was not direct related to frequencies within the expressionless regions, and was therefore not an indicator of a dead region. This therefore suggests that audiograms, and their poor representation of dead regions, are inaccurate predictors of a patient's perception of pure tone quality.[20]
Enquiry by Kluk and Moore has shown that dead regions may also affect the patient's perception of frequencies across the dead regions. There is an enhancement in the power to distinguish betwixt tones that differ very slightly in frequency, in regions just beyond the expressionless regions compared to tones further away. An caption for this may exist that cortical re-mapping has occurred. Whereby, neurons which would normally be stimulated by the expressionless region, have been reassigned to respond to functioning areas near information technology. This leads to an over-representation of these areas, resulting in an increased perceptual sensitivity to small frequency differences in tones.[21]
Vestibulocochlear nervus pathology [edit]
- congenital deformity of the internal auditory culvert,
- neoplastic and pseudo-neoplastic lesions, with special detailed accent on schwannoma of the eighth cranial nerve (acoustic neuroma),
- non-neoplastic Internal Auditory Canal/CerebelloPontine Bending pathology, including vascular loops,
Diagnosis [edit]
Case history [edit]
Before test, a case history provides guidance virtually the context of the hearing loss.
- major business
- pregnancy and childbirth information
- medical history
- development history
- family history
Otoscopy [edit]
Direct examination of the external canal and tympanic membrane (ear drum) with an otoscope, a medical device inserted into the ear culvert that uses lite to examine the condition of the external ear and tympanic membrane, and middle ear through the semi-translucent membrane.
Differential testing [edit]
Differential testing is nigh useful when there is unilateral hearing loss, and distinguishes conductive from sensorineural loss. These are conducted with a low frequency tuning fork, usually 512 Hz, and contrast measures of air and bone conducted sound transmission.
- Weber test, in which a tuning fork is touched to the midline of the forehead, localizes to the normal ear in people with unilateral sensorineural hearing loss.
- Rinne examination, which tests air conduction vs. os conduction is positive, because both os and air conduction are reduced equally.
- less common Bing and Schwabach variants of the Rinne exam.
- absolute os conduction (ABC) test.
Table ane. A table comparison sensorineural to conductive hearing loss
| Criteria | Sensorineural hearing loss | Conductive hearing loss |
| Anatomical site | Inner ear, cranial nerve VIII, or central processing centers | Middle ear (ossicular concatenation), tympanic membrane, or external ear |
| Weber examination | Sound localizes to normal ear in unilateral SNHL | Sound localizes to affected ear (ear with conductive loss) in unilateral cases |
| Rinne exam | Positive Rinne; air conduction > bone conduction (both air and os conduction are decreased every bit, just the difference betwixt them is unchanged). | Negative Rinne; bone conduction > air conduction (os/air gap) |
Other, more complex, tests of auditory role are required to distinguish the different types of hearing loss. Bone conduction thresholds tin can differentiate sensorineural hearing loss from conductive hearing loss. Other tests, such as oto-audio-visual emissions, audio-visual stapedial reflexes, voice communication audiometry and evoked response audiometry are needed to distinguish sensory, neural and auditory processing hearing impairments.
Tympanometry [edit]
A tympanogram is the result of a test with a tympanometer. It tests the part of the center ear and mobility of the eardrum. It can help identify conductive hearing loss due to disease of the heart ear or eardrum from other kinds of hearing loss including SNHL.
Audiometry [edit]
An audiogram is the result of a hearing test. The most mutual type of hearing examination is pure tone audiometry (PTA). It charts the thresholds of hearing sensitivity at a selection of standard frequencies between 250 and 8000 Hz. There is too high frequency pure tone audiometry which tests frequencies from 8000-xx,000 Hz. PTA can be used to differentiate between conductive hearing loss, sensorineural hearing loss and mixed hearing loss. A hearing loss can be described by its caste i.e. mild, moderate, severe or profound, or by its shape i.e. loftier frequency or sloping, low frequency or rising, notched, U-shaped or 'cookie-bite', peaked or apartment.
There are also other kinds of audiometry designed to test hearing acuity rather than sensitivity (voice communication audiometry), or to test auditory neural pathway transmission (evoked response audiometry).
Magnetic resonance imaging [edit]
MRI scans can be used to identify gross structural causes of hearing loss. They are used for congenital hearing loss when changes to the shape of the inner ear or nerve of hearing may assist diagnosis of the crusade of the hearing loss. They are also useful in cases where a tumour is suspected or to determine the degree of impairment in a hearing loss caused by bacterial infection or auto-immune disease. Scanning is of no value in age-related deafness.
Prevention [edit]
Presbycusis is the leading crusade of SNHL and is progressive and nonpreventable, and at this time, we do not have either somatic or factor therapy to counter heredity-related SNHL. But other causes of caused SNHL are largely preventable, especially nosocusis type causes. This would involve fugitive environmental noise, and traumatic dissonance such as rock concerts and nightclubs with loud music. Use of noise attenuation measures similar ear plugs is an alternative, also equally learning almost the noise levels 1 is exposed to. Currently, several authentic sound level measurement apps be. Reducing exposure fourth dimension tin can also aid manage risk from loud exposures.

Treatment [edit]
Handling modalities fall into three categories: pharmacological, surgical, and management. As SNHL is a physiologic degradation and considered permanent, there are as of this time, no approved or recommended treatments.
In that location have been meaning advances in identification of man deafness genes and elucidation of their cellular mechanisms every bit well as their physiological function in mice.[22] [23] Nevertheless, pharmacological treatment options are very express and clinically unproven.[24] Such pharmaceutical treatments every bit are employed are palliative rather than curative, and addressed to the underlying crusade if one can be identified, in order to avert progressive damage.
Profound or total hearing loss may be amenable to direction by cochlear implants, which stimulate cochlear nerve endings directly. A cochlear implant is surgical implantation of a bombardment powered electronic medical device in the inner ear. Unlike hearing aids, which make sounds louder, cochlear implants do the work of damaged parts of the inner ear (cochlea) to provide audio signals to the encephalon. These consist of both internal implanted electrodes and magnets and external components.[25] The quality of sound is different than natural hearing just may enable the recipient to better recognize speech and environmental sounds. Because of risk and expense, such surgery is reserved for cases of severe and disabling hearing impairment
Management of sensorineural hearing loss involves employing strategies to support existing hearing such equally lip-reading, enhanced communication etc. and amplification using hearing aids. Hearing aids are specifically tuned to the private hearing loss to give maximum do good.
Research [edit]
Pharmaceuticals [edit]
- Antioxidant vitamins – Researchers at the Academy of Michigan report that a combination of high doses of vitamins A, C, and E, and Magnesium, taken one hour before racket exposure and continued as a one time-daily treatment for five days, was very effective at preventing permanent racket-induced hearing loss in animals.[26]
- Tanakan – a brand name for an international prescription drug extract of Ginkgo biloba. Information technology is classified every bit a vasodilator. Amongst its research uses is treatment of sensorineural deafness and tinnitus presumed to be of vascular origin.
- Coenzyme Q10 – a substance like to a vitamin, with antioxidant backdrop. It is made in the body, simply levels fall with age.[Note 3]
- Ebselen, a constructed drug molecule that mimics glutathione peroxidase (GPx), a critical enzyme in the inner ear that protects information technology from damage caused by loud sounds or racket [27]
Stem cell and cistron therapy [edit]
Hair cell regeneration using stem jail cell and gene therapy is years or decades away from being clinically feasible.[28] However, studies are currently underway on the discipline, with the first FDA-approved trial start in February 2012.[29]
Sudden sensorineural hearing loss [edit]
Sudden sensorineural hearing loss (SSHL or SSNHL), commonly known as sudden deafness, occurs as an unexplained, rapid loss of hearing—usually in one ear—either at in one case or over several days. Nine out of ten people with SSHL lose hearing in simply ane ear. It should be considered a medical emergency. Delaying diagnosis and treatment may render treatment less constructive or ineffective.
Experts estimate that SSHL strikes ane person per 100 every year, typically adults in their 40s and 50s. The bodily number of new cases of SSHL each year could be much higher because the condition often goes undiagnosed.
Presentation [edit]
Many people notice that they take SSHL when they wake up in the morn. Others first notice information technology when they try to utilise the deafened ear, such equally when they utilize a phone. Still others notice a loud, alarming "pop" just before their hearing disappears. People with sudden deafness frequently get dizzy, have ringing in their ears (tinnitus), or both.
Diagnosis [edit]
SSHL is diagnosed via pure tone audiometry. If the test shows a loss of at least 30 dB in 3 adjacent frequencies, the hearing loss is diagnosed as SSHL. For example, a hearing loss of thirty dB would brand conversational speech audio more than like a whisper.
Causes [edit]
Just 10 to 15 percentage of the cases diagnosed every bit SSHL accept an identifiable cause. Most cases are classified as idiopathic, also called sudden idiopathic hearing loss (SIHL) and idiopathic sudden sensorineural hearing loss (ISSHL or ISSNHL)[30] [31] The majority of show points to some type of inflammation in the inner ear as the nearly common cause of SSNHL.
- Viral – The swelling may exist due to a virus. A herpes type virus is believed to be the most common cause of sudden sensorineural hearing loss. The herpes virus lies dormant in our bodies and reactivates for an unknown reason.
- Vascular ischemia of the inner ear or cranial nerve VIII (CN8)
- Perilymph fistula, usually due to a rupture of the round or oval windows and the leakage of perilymph. The patient will usually also experience vertigo or imbalance. A history of trauma is normally present and changes to hearing or vertigo occur with alteration in intracranial pressure level such as with straining; lifting, blowing etc.
- Autoimmune – tin exist due to an autoimmune illness such as systemic lupus erythematosus, granulomatosis with polyangiitis
Handling [edit]
Hearing loss completely recovers in effectually 35-39% of patients with SSNHL, usually within one to two weeks from onset.[32] Eighty-five per centum of those who receive handling from an otolaryngologist (sometimes called an ENT surgeon) will recover some of their hearing.
- vitamins and antioxidants
- vasodilators
- betahistine (Betaserc), an anti-vertigo drug
- hyperbaric oxygen[33]
- rheologic agents that reduce blood viscosity (such as hydroxyethyl starch, dextran and pentoxifylline)[34]
- anti-inflammatory agents, primarily oral corticosteroids such every bit prednisone, methylprednisone[ citation needed ]
- Intratympanic assistants – Gel formulations are under investigation to provide more consistent drug delivery to the inner ear.[35] Local drug delivery can be accomplished through intratympanic administration, a minimally invasive procedure where the ear pulsate is anesthetized and a drug is administered into the centre ear. From the middle ear, a drug can diffuse across the circular window membrane into the inner ear.[35] Intratympanic administration of steroids may be constructive for sudden sensorineural hearing loss for some patients, merely high quality clinical information has not been generated.[36] Intratympanic administration of an anti-apoptotic peptide (JNK inhibitor) is currently being evaluated in late-phase clinical development.[37]
Epidemiology [edit]
General hearing loss affects close to ten% of the global population.[38] In the The states alone, information technology is expected that xiii.5 million Americans have sensorineural hearing loss. Of those with sensorineural hearing loss, approximately 50% are congenitally related. The other l% are due to maternal or fetal infections, mail-natal infections, viral infections due to rubella or cytomegalovirus, ototoxic drugs,[39] exposure to loud sounds, severe head trauma, and premature births [40]
Of the genetically related sensorineural hearing loss cases, 75% are autosomal recessive, 15-20% autosomal dominant, and 1-three% sexual activity-linked. While the specific factor and protein is still unknown, mutations in the connexin 26 factor most the DFNB1 locus of chromosome thirteen[41] are thought to account for most of the autosomal recessive genetic-related sensorineural hearing loss [40]
At least 8.5 per one thousand children younger than age 18 have sensorineural hearing loss. General hearing loss is proportionally related to historic period. At least 314 per thou people older than age 65 take hearing loss. Several risk factors for sensorineural hearing loss have been studied over the past decade. Osteoporosis, stapedectomy surgery, pneumococcal vaccinations, mobile phone users, and hyperbilirubinemia at nativity are among some of the known run a risk factors.
See also [edit]
- Conductive hearing loss, hearing loss caused primarily past atmospheric condition in the eye ear
- Cortical deafness, another kind of nerve deafness
- Hearing loss
- Inner ear, the innermost portion of the ear containing the sensorineural apparatus of hearing
- Otosclerosis, a sometimes associated or predecessor conductive hearing loss condition of the center ear
- Tinnitus, ringing in the ears, a common accompaniment of SNHL
Notes [edit]
- ^ A few prominent ones are American National Standards Institute (ANSI), International Organization for Standardization (ISO), Deutsches Institut für Normung (DIN), Swedish Standards Establish (SSI), Canadian Standards Clan (CSA), British Standards Found (BSI), Austrian Standards International(ÖNORM), and in the Usa, Environmental Protection Bureau (EPA), Occupational Safe and Wellness Assistants (OSHA) and numerous state agencies, and Department of Defence (DOD) among others.
- ^ The various standards quantify nose exposure with a set of specified measures, ordinarily with respect to a reference exposure time of 8 hours, a typical working day. The measures include, a weighting calibration (normally A) with a sample fourth dimension, a threshold value in dB, a criterion sound pressure level in dB with an exposure fourth dimension usually in hours, and an exchange rate in dB. A weighted SPL is denoted dB(X) where 10 is a weighting scale, normally A, merely sometimes C. (A) refers to A-weighting of SPL, which is an aligning to measured SPL to compensate for the frequency response of the human ear, which is less sensitive to low frequencies. The criterion level is the average sound force per unit area level permitted over the exposure time. The threshold sound pressure level is the level to a higher place which sound will exist integrated into the average. The sample time (fast, slow or impulse) is the charge per unit of sampling — a slow sample time is 1 2nd; a fast sample time is one/viii second, and impulse sample time is 35 milliseconds. The effect of a slower sample fourth dimension ways that very short elapsing sounds may not be fully sampled (or even sampled at all in rare cases), so the dissonance exposure may be underestimated. The substitution rate is the amount by which the permitted sound level may increase if the exposure time is halved.
- ^ Coenzyme Q10(CoQ10) supports mitochondrial part and has pregnant antioxidant backdrop (Quinzii 2010). Animal studies have found that supplementation with CoQ10 reduced dissonance-induced hearing loss and the death of pilus cells (Hirose 2008; Fetoni 2009, 2012). Human studies have also yielded promising results, every bit 160-600 mg of CoQ10 daily was found to reduce hearing loss in people with sudden sensorineural hearing loss and presbycusis (Ahn 2010; Salami 2010; Guastini 2011). Likewise, a small-scale preliminary trial found that CoQ10 supplementation alleviated tinnitus in those whose CoQ10 blood levels were initially low (Khan 2007). Another small trial found CoQ10 may slow progression of hearing loss associated with a mitochondrial genetic mutation (Angeli 2005).
References [edit]
- ^ Newman CW, Weinstein Be, Jacobson GP, Hug GA (Oct 1991). "Test-retest reliability of the hearing handicap inventory for adults". Ear and Hearing. 12 (5): 355–seven. doi:ten.1097/00003446-199110000-00009. PMID 1783240.
- ^ Matsunaga T (Dec 2009). "Value of genetic testing in the otological approach for sensorineural hearing loss". The Keio Journal of Medicine. 58 (4): 216–22. doi:10.2302/kjm.58.216. PMID 20037285.
- ^ Papadakis CE, Hajiioannou JK, Kyrmizakis DE, Bizakis JG (May 2003). "Bilateral sudden sensorineural hearing loss caused past Charcot-Marie-Tooth disease". The Periodical of Laryngology and Otology. 117 (five): 399–401. doi:10.1258/002221503321626465. PMID 12803792.
- ^ Crispino JD, Horwitz MS (April 2017). "GATA factor mutations in hematologic disease". Blood. 129 (15): 2103–2110. doi:ten.1182/claret-2016-09-687889. PMC5391620. PMID 28179280.
- ^ Hirabayashi S, Wlodarski MW, Kozyra E, Niemeyer CM (August 2017). "Heterogeneity of GATA2-related myeloid neoplasms". International Journal of Hematology. 106 (2): 175–182. doi:ten.1007/s12185-017-2285-2. PMID 28643018.
- ^ Mills JH, Going JA (April 1982). "Review of environmental factors affecting hearing". Environmental Wellness Perspectives. 44: 119–27. doi:10.1289/ehp.8244119. PMC1568958. PMID 7044773.
- ^ Rosen, S.; Bergman, M.; Plester, D.; El-Mofty, A.; Satti, M. H. (September 1962). "Presbycusis written report of a relatively noise-free population in the Sudan". The Register of Otology, Rhinology, and Laryngology. 71 (iii): 727–743. doi:10.1177/000348946207100313. ISSN 0003-4894. PMID 13974856. S2CID 30150198.
- ^ Goycoolea, M. V.; Goycoolea, H. One thousand.; Farfan, C. R.; Rodriguez, L. G.; Martinez, K. C.; Vidal, R. (December 1986). "Effect of life in industrialized societies on hearing in natives of Easter Island". The Laryngoscope. 96 (12): 1391–1396. doi:10.1288/00005537-198612000-00015. ISSN 0023-852X. PMID 3784745. S2CID 23022009.
- ^ Salawati, Liza (2012). Le Prell, Colleen G.; Henderson, Donald; Fay, Richard R.; Popper, Arthur Due north. (eds.). Racket-Induced Hearing Loss. Jurnal Kedokteran Syiah Kuala. Springer Handbook of Auditory Inquiry. Vol. 40. pp. 45–49. doi:ten.1007/978-ane-4419-9523-0. ISBN978-1-4419-9522-3. S2CID 6752992.
- ^ Gates GA, Mills JH (September 2005). "Presbycusis". Lancet. 366 (9491): 1111–xx. doi:10.1016/S0140-6736(05)67423-5. PMID 16182900.
Presbycusis (or presbyacusis) is a full general term that refers to hearing loss in the elderly and, as such, represents the contributions of a lifetime of insults to the auditory system. Of these, ageing and noise harm are the master factors, plus genetic susceptibility, otological disorders, and exposures to ototoxic agents.
- ^ "Audio Output Levels of the iPod and Other MP3 Players: Is There Potential Risk to Hearing?". Archived from the original on October xxx, 2007. Retrieved 2007-11-twenty .
- ^ Kochupillai North, Pandav CS, Godbole MM, Mehta M, Ahuja MM (1986). "Iodine deficiency and neonatal hypothyroidism". Bulletin of the World Health Organization. 64 (iv): 547–51. PMC2490891. PMID 3490923.
- ^ a b c d due east f Gelfand SA. Hearing: An Introduction to Psychological and Physiological Acoustics. quaternary ed. New York: Marcel Dekker; 2004.
- ^ a b c d e f g h i j grand Moore BCJ. Cochlear Hearing Loss. London: Whurr Publishers; 1998.
- ^ a b c d e f Moore BC (April 2004). "Dead regions in the cochlea: conceptual foundations, diagnosis, and clinical applications". Ear and Hearing. 25 (2): 98–116. doi:10.1097/01.aud.0000120359.49711.d7. PMID 15064655. S2CID 12200368.
- ^ Terkildsen K (1980). "Hearing damage and audiograms". Scand Audiol. ten: 27–31. Cited in: Moore BC (March 2001). "Expressionless regions in the cochlea: diagnosis, perceptual consequences, and implications for the plumbing equipment of hearing AIDS". Trends in Amplification. five (i): 1–34. doi:10.1177/108471380100500102. PMC4168936. PMID 25425895.
- ^ Thornton AR, Abbas PJ, Abbas PJ (February 1980). "Low-frequency hearing loss: perception of filtered speech, psychophysical tuning curves, and masking". The Journal of the Acoustical Society of America. 67 (2): 638–43. Bibcode:1980ASAJ...67..638T. doi:ten.1121/1.383888. PMID 7358904. Cited in: Moore BC (March 2001). "Expressionless regions in the cochlea: diagnosis, perceptual consequences, and implications for the fitting of hearing AIDS". Trends in Distension. 5 (1): one–34. doi:10.1177/108471380100500102. PMC4168936. PMID 25425895.
- ^ a b c d Sek A, Alcántara J, Moore BC, Kluk K, Wicher A (July 2005). "Development of a fast method for determining psychophysical tuning curves". International Journal of Audiology. 44 (7): 408–twenty. doi:10.1080/14992020500060800. PMID 16136791. S2CID 144611882.
- ^ a b Summers V, Molis MR, Müsch H, Walden BE, Surr RK, Cord MT (April 2003). "Identifying dead regions in the cochlea: psychophysical tuning curves and tone detection in threshold-equalizing noise". Ear and Hearing. 24 (2): 133–42. doi:10.1097/01.AUD.0000058148.27540.D9. PMID 12677110. S2CID 35548604.
- ^ Huss M, Moore BC (October 2005). "Dead regions and noisiness of pure tones". International Journal of Audiology. 44 (ten): 599–611. doi:10.1080/02640410500243962. PMID 16315451. S2CID 46489920.
- ^ Kluk Thou, Moore BC (December 2006). "Dead regions in the cochlea and enhancement of frequency discrimination: Effects of audiogram slope, unilateral versus bilateral loss, and hearing-aid apply". Hearing Inquiry. 222 (1–2): i–xv. doi:10.1016/j.heares.2006.06.020. PMID 17071031. S2CID 31883892.
- ^ Safieddine S, El-Amraoui A, Petit C (2012). "The auditory hair cell ribbon synapse: from assembly to function". Almanac Review of Neuroscience. 35: 509–28. doi:10.1146/annurev-neuro-061010-113705. PMID 22715884.
- ^ Wichmann C, Moser T (July 2015). "Relating structure and function of inner hair cell ribbon synapses". Jail cell and Tissue Research. 361 (i): 95–114. doi:x.1007/s00441-014-2102-7. PMC4487357. PMID 25874597.
- ^ Nakagawa T (2014). "Strategies for developing novel therapeutics for sensorineural hearing loss". Frontiers in Pharmacology. v: 206. doi:10.3389/fphar.2014.00206. PMC4165348. PMID 25278894.
- ^ "Sensorineural Hearing Loss". HealthCentral. Retrieved 8 June 2013.
- ^ "Nutrients Prevent Racket Induced Hearing Loss". 2013-05-08. Archived from the original on viii May 2013. Retrieved 2016-02-25 .
- ^ "Audio Pharmaceuticals submits positive Phase 2 clinical trial data on SPI-1005 for the... - SEATTLE, February. 18, 2014 /PRNewswire/". Prnewswire.com . Retrieved 2016-02-25 .
- ^ Parker MA (Dec 2011). "Biotechnology in the treatment of sensorineural hearing loss: foundations and future of pilus cell regeneration". Journal of Speech, Linguistic communication, and Hearing Research. 54 (6): 1709–31. doi:10.1044/1092-4388(2011/x-0149). PMC3163053. PMID 21386039.
- ^ "Written report Using Stem Cells to Treat Sensorineural Hearing Loss Underway". HealthyHearing. 2 February 2012. Retrieved viii June 2013.
- ^ "Sudden Deafness | Massachusetts Eye and Ear". Masseyeandear.org . Retrieved 2016-02-25 .
- ^ "H91.2". ICD-10 Version:2010. apps.who.int. 2010.
- ^ Bayoumy, AB; van der Veen, EL; de Ru, JA (ane Baronial 2018). "Cess of Spontaneous Recovery Rates in Patients With Idiopathic Sudden Sensorineural Hearing Loss". JAMA Otolaryngology–Head & Neck Surgery. 144 (8): 655–656. doi:10.1001/jamaoto.2018.1072. PMID 29931029. S2CID 49330911.
- ^ Bennett MH, Kertesz T, Perleth M, Yeung P, Lehm JP (Oct 2012). "Hyperbaric oxygen for idiopathic sudden sensorineural hearing loss and tinnitus". The Cochrane Database of Systematic Reviews. x: CD004739. doi:10.1002/14651858.CD004739.pub4. PMID 23076907.
- ^ Li, Yike (15 June 2017). "Interventions in the management of blood viscosity for idiopathic sudden sensorineural hearing loss: A meta-analysis". Journal of Wellness Research and Reviews. iv (2): l–61. doi:10.4103/jhrr.jhrr_125_16. S2CID 79662388.
- ^ a b McCall AA, Swan EE, Borenstein JT, Sewell WF, Kujawa SG, McKenna MJ (Apr 2010). "Drug delivery for treatment of inner ear disease: current land of noesis". Ear and Hearing. 31 (2): 156–65. doi:10.1097/AUD.0b013e3181c351f2. PMC2836414. PMID 19952751.
- ^ Crane RA, Camilon 1000, Nguyen S, Meyer TA (January 2015). "Steroids for treatment of sudden sensorineural hearing loss: a meta-analysis of randomized controlled trials". The Laryngoscope. 125 (1): 209–17. doi:10.1002/lary.24834. PMID 25045896. S2CID 24312659.
- ^ Suckfuell 1000, Lisowska One thousand, Domka Westward, Kabacinska A, Morawski K, Bodlaj R, Klimak P, Kostrica R, Meyer T (September 2014). "Efficacy and rubber of AM-111 in the handling of acute sensorineural hearing loss: a double-blind, randomized, placebo-controlled stage Two report". Otology & Neurotology. 35 (8): 1317–26. doi:10.1097/mao.0000000000000466. PMID 24979398. S2CID 6445497.
- ^ Oishi, Naoki; Schacht, Jochen (2011). "Emerging treatments for dissonance-induced hearing loss". Expert Opinion on Emerging Drugs. sixteen (2): 235–245. doi:10.1517/14728214.2011.552427. ISSN 1472-8214. PMC3102156. PMID 21247358.
- ^ "Genetic Sensorineural Hearing Loss: Groundwork, Pathophysiology, Epidemiology". 2019-11-09.
- ^ a b Antonio, Stephanie (2018-06-12). "Genetic Sensorineural Hearing Loss Clinical Presentation". Medscape.
- ^ "Welcome to the Hereditary Hearing Loss Homepage | Hereditary Hearing Loss Homepage". hereditaryhearingloss.org . Retrieved 2019-12-03 .
38.Ghazavi H,Kargoshaei A-A,Jamshidi-Koohsari One thousand,"Investigation of vitamin D levels in patients with Sudden Sensory-Neural Hearing Loss and its result on treatment",American journal of otolaryngology and caput and neck medicine and suegery,Nov 2019 https://doi.org/10.1016/j.amjoto.2019.102327
External links [edit]
- Hearing Loss Web

Definition Of A Perceptual Region,
Source: https://en.wikipedia.org/wiki/Sensorineural_hearing_loss
Posted by: jacksonhipild.blogspot.com
0 Response to "Definition Of A Perceptual Region"
Post a Comment